

Hearing loss occurs when the ability to hear is impaired as compared to someone with normal hearing. Humans have the ability to detect sounds from a range of frequency from 20Hz to 20kHz while its loudness is measured in decibel (dB). A normal hearing for each frequency is defined as having a hearing threshold of 25dB or better. Some level of hearing loss is said to occur below this threshold.
Hearing loss can be mild (26- 40dB), moderate (41dB-55dB), moderately severe (56-70dB), severe (71-90dB) and profound (>91dB). Deafness in a ear usually refers to at least a profound or total hearing loss.
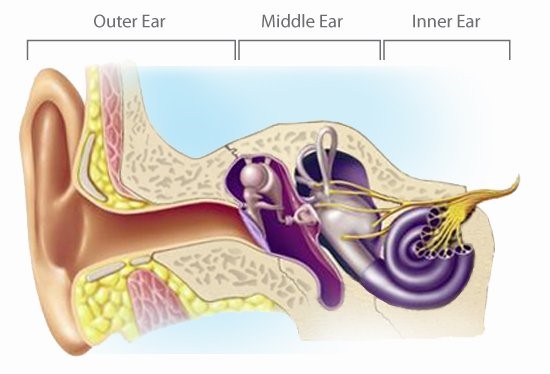
Our ear is divided into 3 parts which are outer, middle and inner ear. The outer and middle ear are responsible for conducting and amplifying the sound from the environment while the inner ear is responsible for converting mechanical sound energy into electrical impulses to be sent for processing in the auditory cortex of the brain. Hearing loss can occur when there is disruption in the conduction of sound due to problems of the outer and middle ear which results in Conductive type Hearing Loss. Pathology in the inner ear will result in a Sensorineural type Hearing Loss. A combination of both conductive and sensorineural type hearing loss is referred to as Mixed Hearing Loss.
The most common cause of conductive hearing loss is impacted ear wax in the outer ear. Other common conditions that cause conductive hearing loss include:
Outer ear : otitis externa (swollen ear canal), foreign body or congenital causes such as ear canal atresia (failure of normal external ear development).
Middle ear : middle ear effusion / otitis media (fluid in the middle ear), ossicular dislocation from trauma and otosclerosis
For sensorineural hearing loss, the most common cause is due to presbyacusis (degeneration from aging). In the adult, it can also happen from damage to the inner ear as a result of prolonged exposure to noise hazard which can be work related, head injury or ototoxicity (drug induced).
Sensorineural hearing loss can also occur in a child. In such cases, it could either be congenital (from birth) or developmental (after birth). Conditions that can cause sensorineural hearing loss in a child include prematurity, certain syndromes with craniofacial anomalies, meningitis and hyperbilirubinaemia (jaundice).
Presentation of a person with hearing loss depends on the age. A child with hearing loss may present with speech delay or other learning disability while an adult may have difficulty in communication while also speaking inappropriately loud. Having hearing impairment is also shown to have an effect on an individual’s self-confidence. This would lead to social withdrawal and depression. Tinnitus (ringing in the ear) is also a common symptom in patients with hearing loss.
While newborn hearing screening is commonly done before discharge, parents need to be always vigilant if they suspect any hearing loss in their child. This is because the speech language development is most crucial in the first 2 years of a child’s life. The earlier it is recognised, the earlier intervention could be instituted, the better the chances of normal development for the child. This is especially for child who may have bilateral (both ear) deafness and may require a cochlear implant.
One should also be aware that hearing loss could also be only a part of a symptom of a more sinister underlying health diagnosis. A unilateral (one sided) ear block sensation that does not resolve over a week warrant further assessment as it could also be an early symptom of NPC (nasopharyngeal carcinoma) due to the mass in the nasopharynx obstructing the Eustachian tube opening. Sinusitis can also cause similar type hearing loss although it is usually transient while a child with persistent middle ear effusion may be caused by an underlying adenoid hypertrophy.
To diagnose hearing loss in an adult, a pure tone audiogram is commonly performed to assess the level and severity of the hearing loss. For a younger child, a BSER (Brainstem evoked response) to detect the brain wave activity to a given sound stimulus is preferred.
Management of hearing loss depends on the cause. Clearing of impacted ear wax may resolve the hearing loss. Middle ear effusion may be treated medically or if persist surgically with myringotomy and grommet insertion. Hearing loss that still persists or of sensorineural type may require the use of hearing aid if the hearing loss in indeed impairing quality of life. Types of hearing aid depends on an individual’s level of hearing loss, preference and dexterity in handling the smaller type hearing aid.
For a child found to have bilateral profound hearing loss, a cochlear implant early in a child’s speech language development would be crucial for the best outcome.
Optimal management of hearing loss also aims to restore binaural hearing. Binaural hearing (hearing with both ears) has the advantage of localising the direction of a sound. Hence, a person with single sided hearing loss may have difficulties in determining the direction of sound as well as reduced sound clarity.

Non medical treatment of hearing loss aims at prevention as well as to slow its progress. Individuals should practice good ear care in avoiding prolonged exposure to loud noises which can damage the inner ear’s hair cells. Earplugs should be used if noise hazard in the work environment cannot be avoided. Consumption of certain vitamin supplements may also help to slow the progress of nerve degeneration.
For more information on hearing loss or other medical issues, please surf to https://www.srikotamedical.com/




{kind=link}